Salivary gland malignancy
OLGU ÖZETİ
Hasta
59, Yaş kadınTanı
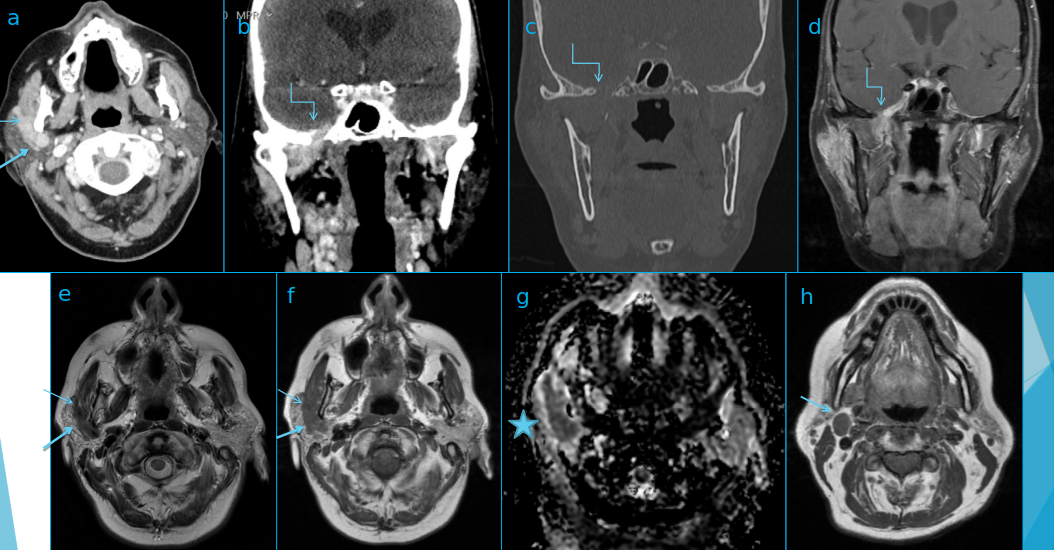
Upper row - axial CT with contrast (a)- coronar CT with contrast (b)- coronar CT bone window (c)- T1 coronal with contrast and fat sat (d)Lower row- T2 axial (e)- T1 axial (f)- ADC map (g)- T1 axial at the level of IIa lymph nodes (h)Yazar
Dr. Beatrix Kovácsovics - University Hospital Linköping SwedenTarih
08/10/2020MR BULGULARI
TARTIŞMA
Differential diagnoses:
- Benign mixed tumor, aka pleomorphic adenoma
-Carcinoma ex pleomorphic adenoma with perineural spread
-Whartin tumor
-Salivary gland malignancy with perineural spread
- Non Hodgkin lymphoma with perineural spread
Cranial nerves involved:
- Facial nerve and maxillary nerve
- Facial nerve and mandibular nerve
- Facial nerve and ophthalmic nerve
- Facial nerve and glossopharyngeal nerve
Diagnosis
- Salivary gland malignancy
- (Adenoid cystic cancer according to pathology)
- Perineural spread along facial and mandibular nerves
- Lymph node metastasi
Imaging findings
- contrast enhancing mass in the right parotid gland (thick arrow a,e,f)
- growing along the facial (thin arrow, a,e,f)
- and mandibular nerves (zigzag arrow b,c,d)
- foramen ovale is widened and the tumor extends intracranially up to the cavernous sinus (zigzag arrow b,c,d)
- the mass has low signal on T2 low ADC value (star on g).
- metastatic lymph node (medium arrow, h)
Benign mixed tumor, aka pleomorphic adenoma
- Benign tumor arising from distal portions of parotid ductal system
- Manifests as painless cheek mass
- Patients are usually older than 40 years
- T2 signal can be very high, higher than CSF, ADC values are high
- Signal in bigger tumors can be heterogenous due to necrosis, hemorrhage and calcification
- Dynamic contrast MRI shows quick uptake then plateau
Carcinoma ex pleomorphic adenoma
- Rapid enlargement of longstanding parotid mass
- Facial nerve weakness and pain
- Early tumor: indistinguishable from benign mixed tumor
- Late tumor: aggressive, infiltrating parotid mass
- T2 signal is higher than other tumors
Whartin tumor
- Painless mass in the parotid tail (angle of the mandible)
- 90% of the patients with this tumor is smoker
- 20% of cases can be multiple masses
- Sharply marginated, heterogenic mass
- Lesion is most conspicuous on STIR sequence
- ADC value is similar to cancer
- Takes up FDG
Salivary gland malignancy with perineural spread
- (mucoepidermoid cancer or adenoid cystic carcinoma)
- Malignant tumors arising from the parotid ducts
- Manifests as palpable, hard, painful parotid mass
- Often combined with cranial nerve symptoms (ex. facial nerve palsy)
- T2 signal is lower than benign tumor´s
- Always look after perineural tumor growth
Non-Hodgkin lymphoma with perineural spread
- Slowly enlarging parotid mass with our without nodes on the neck
- Patient may have systemic “B” symptoms
- Different imaging features for nodal and primary parenchymal lymphoma
- Intermediate or low T2 signal, low ADC value
- FDG avid (MALT lymphoma is not so FDG avid)
Connections between trigeminal and facial nerves
- Parotid gland: auriculotemporal nerve (V/3) & facial nerve
- High masticator space: lingual nerve (V/3) & chorda tympani
- Otic ganglion under skull base: V/3 & lesser petrosal nerve
- Pterygopalatine fossa: two pterygopalatine nerves from V/2 & Vidian nerve (n petrosus maior)
KAYNAKLAR
MR GÖRÜNTÜLERİ